Minimally Invasive Knee Surgery: How Procedures Are Performed And Who May Benefit
Surgical techniques and instrumentation used in minimally invasive knee surgery
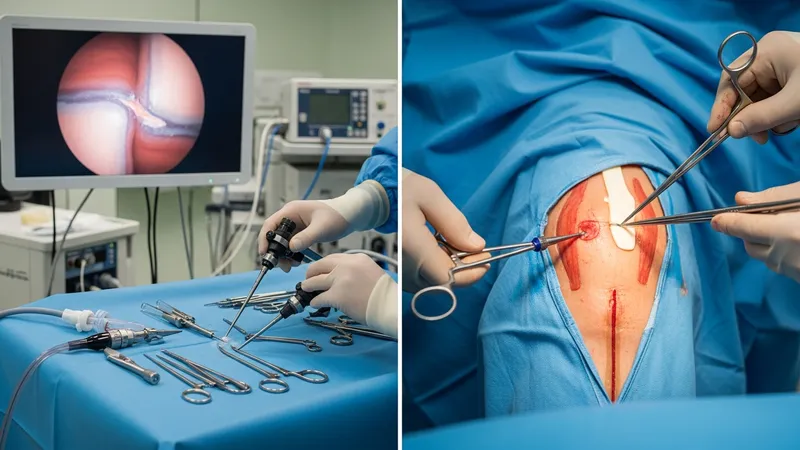
Arthroscopic techniques use small portals—typically 4–8 mm—through which an arthroscope and working instruments access the joint. Visualization relies on a camera system that projects magnified images onto a monitor, allowing precision work in confined spaces. Instruments designed for these portals include shavers, graspers, knotless anchors, and specialized suturing devices for meniscal repair. Surgeons may employ fluid management systems to maintain clear visualization and hemostasis. Portal positioning is planned to balance direct access to pathology with avoidance of nearby neurovascular structures.
Mini-open partial knee replacement involves a reduced-length incision over the affected compartment with preservation of uninvolved ligaments and surrounding tissue. Specialized retractors, narrow trial components, and scaled instruments facilitate component alignment and fixation through the smaller exposure. Some teams incorporate intraoperative imaging or alignment guides to verify implant position. When robotic or navigation adjuncts are used, the goal is to enhance component placement precision while retaining the minimally invasive exposure, though these adjuncts add equipment and setup considerations.
Ligament reconstruction techniques using arthroscopic assistance combine portal-based visualization with small-incision graft harvest or tunnel creation. Graft passage and fixation often rely on specific fixation devices that can be deployed through limited access. Cartilage restoration procedures such as microfracture, autologous chondrocyte implantation, or osteochondral grafting can also be adapted to smaller exposures when lesions are focal. The choice of instruments and fixation methods is matched to lesion size, location, and tissue quality to optimize handling within a constrained operative field.
Technology choices—arthroscopes, radiofrequency devices, or biologic adjuncts—affect intraoperative workflow and inventory needs. Surgeons and surgical teams typically select systems based on familiarity, evidence base, and institutional availability. Sterile technique and careful instrument management are particularly important in minimally invasive approaches because small portals offer limited redundancy for access; efficient instrument exchange and clear visualization help reduce operative time and potential complications.