Minimally Invasive Knee Surgery: How Procedures Are Performed And Who May Benefit
Minimally invasive knee procedures use smaller incisions, specialized instruments, and targeted visualization to address joint problems while limiting disruption of surrounding tissue. Rather than wide exposure, surgeons typically access the knee through portals or reduced-length cuts and use arthroscopic cameras, narrow retractors, and precision tools to inspect and treat cartilage, meniscal tears, ligament injuries, or a single compartment of the joint. The approach aims to maintain the joint’s structural integrity and permit focused correction of the identified pathology while reducing visible scarring and surgical footprint compared with larger open methods.
Patient selection and preoperative assessment are central to deciding whether a less invasive approach may be appropriate. Clinicians often consider imaging findings, symptom patterns, alignment of the limb, activity goals, and overall health. Some conditions that are localized or limited in extent may be amenable to smaller-access techniques, whereas diffuse arthritis or complex multi-ligament damage can require more extensive exposure. Preoperative planning typically includes radiographs, MRI or CT as needed, and discussion of realistic postoperative expectations with the treating team.
- Arthroscopic diagnostic and therapeutic procedures — small-portal techniques for meniscal repair, debridement, loose body removal, and synovial inspection that use an arthroscope and narrow instruments.
- Mini-open unicompartmental (partial) knee replacement techniques — reduced-incision methods to replace a single damaged compartment with preservation of unaffected compartments and ligaments.
- Arthroscopic ligament reconstruction and cartilage restoration methods — techniques using small incisions for graft tunnels, anchor placement, or biologic augmentation to address focal instability or cartilage defects.
Comparisons among these approaches often focus on scope and goals rather than absolute superiority. Arthroscopic procedures are frequently chosen for focal intra-articular problems because they allow direct visualization with minimal soft-tissue disruption. Mini-open partial replacement is a different category, involving joint-surface replacement through a smaller exposure when disease is limited to one compartment. Ligament reconstructions using arthroscopic assistance may combine small portals with targeted graft tunnels. Each modality may vary in intraoperative time, instrument needs, and postoperative protocols, so clinicians weigh these practical differences case by case.
Indications and contraindications are assessed on individual grounds and often emphasize anatomy and disease extent. For instance, isolated meniscal tears in structurally stable knees may be suited to arthroscopic repair or trimming, whereas widespread degenerative change across multiple compartments may not be suitable for limited exposure techniques. Patient factors such as body habitus, prior surgeries, systemic conditions, and expectations about recovery generally influence the choice of approach. Imaging and clinical examination are used together to form a balanced judgment about whether a less invasive approach may be feasible.
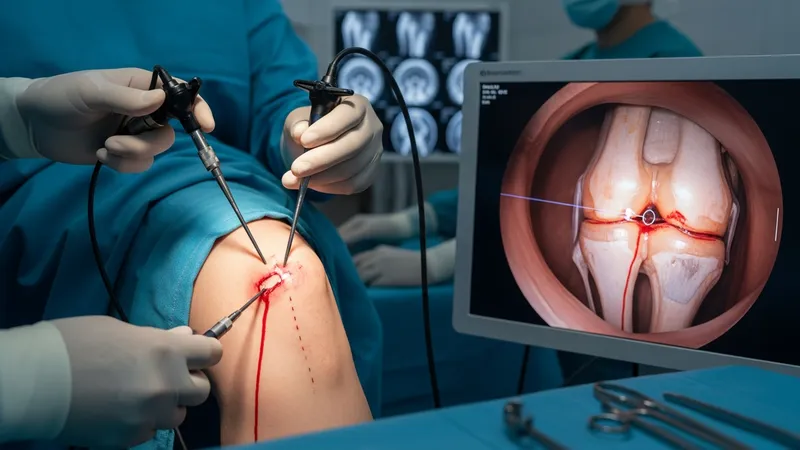
Intraoperative technique considerations typically involve portal placement, instrument trajectory, and visualization strategy. Surgeons commonly plan portals to optimize access to the affected compartment while avoiding neurovascular structures. Visualization relies on streaming arthroscopic camera images or magnified views, and instruments are selected for length, curvature, and function appropriate to the task. In cases of partial replacement, alignment guides and trial components are used through the smaller incision to verify fit. Technology such as dedicated retractors or endoscopic lighting can support these techniques without changing the underlying surgical principles.
Recovery patterns after less invasive knee procedures can vary by procedure type and patient baseline. Pain control protocols may combine multimodal analgesia and local infiltration techniques to reduce opioid exposure. Weight-bearing and range-of-motion progression are often individualized: some arthroscopic procedures permit immediate weight-bearing as tolerated, whereas partial replacement may include staged loading and physiotherapy. Rehabilitation plans typically emphasize progressive strengthening, mobility, and functional milestones over weeks to months, and clinical follow-up monitors wound healing, pain trajectory, and functional gains.
Overall, minimally invasive knee methods encompass a range of targeted techniques that may be applicable when pathology is focal and patient factors align with the approach. Surgical planning usually integrates imaging, clinical findings, and instrumentation choices to balance operative access with tissue preservation. The next sections examine practical components and considerations in more detail.